January 2012
Length Associated Muscle Changes: The Cascade to Dysfunction
By: Jason Martuscello
The evolution of technology has marveled the world in many ways. Advancements such as cutting edge fitness equipment, to the computer you are reading this from all help serve their function and purpose. To optimize these tools to provide an effective and efficient outcome one must become educated with its detail to function. However, this requires time and patience. Furthermore this becomes more difficult to accomplish as technology is constantly changing. Although dealing with changes regularly may create frustration, the concept of muscle function and mechanics of the body do not change2. Although the functions remain constant, we still deal with an abundance of musculoskeletal disorders signifying the lack of appreciation in the finer details of muscle function and body mechanics.
In an effort to prevent the musculoskeletal problems experienced, a large focus has been directed toward performing
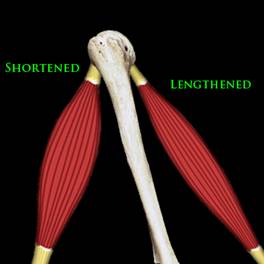 |
Figure 1: Muscular Imbalance |
functional movement in opposition of dysfunctional movement patterns. Many programs, training regiments, and theories have been designed to rid the body of flawed movements that lead to : muscular imbalances, postural deviations, and asymmetries. Understanding the causes of dysfunctional movements is a prerequisite to assess, prescribe exercise, and design programs that alleviate movement flaws and optimize function.
Muscle balance is essential for normal function. Furthermore providing efficient movement of the musculoskeletal system is reliant on optimal muscle function. Optimal function is achieved through proper length tension relationships to allow appropriate force production, activation timing, and timing duration1. Muscle balance can be defined as the equality of muscle length or strength between an agonist and antagonist. When in balance, the opposing forces properly keep the bones centered under joint motion3. In other words, imbalance can be defined as a disproportion in length or strength of two opposing muscle structures (Figure 1).
Structural & Functional Approach
Much of our understanding of muscular imbalances can be credited to the pioneering work of Janda, Kendall, and
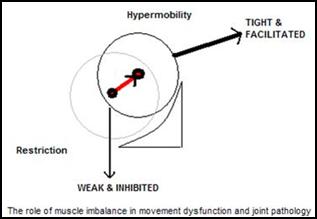 |
| Figure 2: joint Mobility with Length Associated Changes |
Sahrmann. Kendall2 and Sahrmann4 popularized the biomechanical basis (Structural Approach) of imbalances through repetitive movements and sustaining static postures for durations. These movement patterns contribute to structural changes within in muscle producing length alterations at the sarcomere level of muscle. Within the structural approach, Sahrmann4 highlighted the concept of relative flexibility and stiffness1. Length associated changes in muscles causing “relative flexibility” and “relative stiffness” ultimately affect the joint range of motion (Figure 2). Janda5 popularized the neurological imbalance amongst the inseparable interaction of the central nervous system and musculoskeletal system predisposing muscle groups to be tight or weak.
KENDALL’s MODEL - Structural |
Adaptive Shortening |
Stretch Weakness |
Multi-Articular Muscles |
Mono-Articular Muscles |
- Muscle remaining in a Shortened Position
|
- Weakness Due to Elongation
- Beyond Normal Resting Length
- *Duration Dependent, Not Severity Dependent
|
Two Joint Muscles |
One Joint Muscles |
JANDAS MODEL - Neurological |
Postural (Tonic) Muscles |
Phasic Muscles |
Shortened Two Joint |
Weakened One Joint |
Prone to Tightness or Shortness |
Prone to Weakness or Inhibition |
Repetitive or Rhythmic Activity |
Work Eccentrically Against Gravity |
SAHRMANN MODEL |
Relative Flexibility |
Relative Stiffness |
Multi-Articular Muscles |
Mono-Articular Muscles |
- Lack Extensibility
- Generate Excessive Tension
|
- Lack Ability to Shorten
- Lengthened or Strained
- Demonstrate Weakness
|
Limit Normal Motion
(Compensated in Movement System) |
Allow Excessive Motion at a Joint |
TABLE 1: Summary of Kendall, Sahrmann & Janda's Work
Where Length Associated Changes Develop
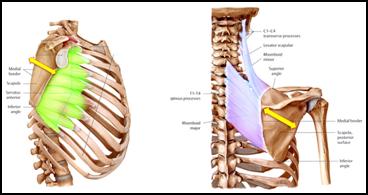
The body constantly strives to maintain balance. When imbalances exist compensation must arise to maintain equilibrium. Compensation often arises between cocontracting muscle structures known as synergists (otherwise known as force couples) or opposing contracting structures known as antagonistic muscles. Synergistic muscles work simultaneously to control movement, joint position, or body part6 (See Figure 3 & 4 for examples). Antagonistic muscles work in an opposing manor where one contracts and the other relaxes. For example, in performing a bicep curl the biceps brachii contracts and shortens as the triceps brachii relaxes and lengthens.
 |
|
Figure 3: Synergist Action Stabilizing the Scapula |
Figure 4: Synergistic Action for Lower Extremity Movement |
When muscular imbalances exist the complimentary muscle structures do not function properly producing dysfunctional movement patterns. The harmonious antagonistic contraction and relaxation cycles become disrupted and coordinated synergistic muscles cocontract asynchronously.
How Length Changes Develop
It may seem obvious to restore, preserve, and improve function of the body it must be rid of imbalances. Although it may seem vital to correct the potential movement flaws first - the initial goal should be familiarizing oneself with how they developed. To reemphasize my point, I cite the famous idiom spoken by Benjamin Franklin, “an ounce of prevention is worth a pound of cure.” Therefore, creating balance within the body the process can be twofold – preventing  the imbalance and restoring balance. To further clarify my point, take the example of trying to lose weight. It does not matterthe amount one exercises if they counterbalance their hard work through an overconsumption of food. Likewise, we arenot going to rid the body of muscular imbalances if one takes no effort to prevent them from occurring in the first place. To understand how and when muscular imbalances exist, a mindset should be adopted that the body is constantly being trained by the postures you maintain. How you sit, stand, walk, sleep, exercise and the alignment your body maintains during these types of activities is how the body is trained and adapts. The position the muscles adapt to has become known as muscles functional resting length or neutral physiological resting position1. Therefore, maintaining a muscle in a lengthened or shortened position has been associated with overall length changes in muscle7,8. In summary, imbalances are developed through constant or repetitive postures or movements assumed in all aspects of living. Other imbalances can be credited to trauma or injury, or immobilization (ie. Cast, Brace)7 the imbalance and restoring balance. To further clarify my point, take the example of trying to lose weight. It does not matterthe amount one exercises if they counterbalance their hard work through an overconsumption of food. Likewise, we arenot going to rid the body of muscular imbalances if one takes no effort to prevent them from occurring in the first place. To understand how and when muscular imbalances exist, a mindset should be adopted that the body is constantly being trained by the postures you maintain. How you sit, stand, walk, sleep, exercise and the alignment your body maintains during these types of activities is how the body is trained and adapts. The position the muscles adapt to has become known as muscles functional resting length or neutral physiological resting position1. Therefore, maintaining a muscle in a lengthened or shortened position has been associated with overall length changes in muscle7,8. In summary, imbalances are developed through constant or repetitive postures or movements assumed in all aspects of living. Other imbalances can be credited to trauma or injury, or immobilization (ie. Cast, Brace)7
What happens when imbalances exist?
It may be familiar that imbalances eventually cause disruption within our movement system. What is not clear is to how a shortened and lengthened muscle can cause all these issues. The understanding in the finer details causing alteration of muscle function due to length-associated changes is quite complex. Although, understanding these fundamental concepts will ultimately better you efforts to preventing issues and restoring balance.
The function of muscle cannot be accomplished without the interdependence of the central nervous system and the musculoskeletal system5. When imbalances exist, compensation arises through alternations in anatomical, biochemical, and physiological properties of skeletal muscle7. Anatomical changes are seen with length changes adapting to meet an individual’s habitual contractile needs or maintained postures. Biochemical alterations in enzyme activity have been documented within length changes. Physiological changes are a result of altering the skeletal muscles ability to develop peak tension7.
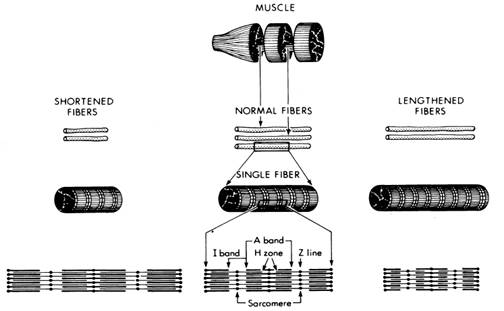
The sarcomere is considered the functional unit of skeletal muscle fibers being responsible for the mechanics of muscle contraction9. The functional properties of skeletal muscle can be determined by sarcomere length. As discussed previously, when an imbalance exists muscles are lengthened and shortened7.
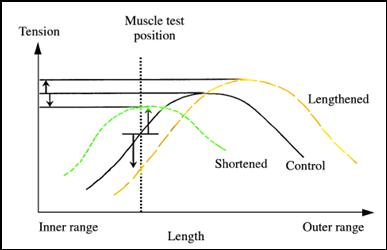 |
Figure 5: Muscle Length and Peak Tension Development *Adapted from Comerford & Mottram1 |
In shortened muscles, sarcomeres are lost and the remaining sarcomeres are stretched to compensate8. In lengthened muscles, sarcomeres are added and will reduce in length8. These anatomical changes will further lead to physiological alterations as well as biochemical. As sarcomeres change in number and in size the ability of the muscle contraction to reach peak tension is altered7. Shorter muscles developing peak tension earlier2 (inner range) while showing less peak tension development8. Lengthened muscles develop peak tension in the outer range confirming Kendall’s ‘stretch weakness concept7 (See Figure 5). Therefore altered length tension relationships result in the different ranges the muscles can produce maximal force. The distributed ranges of development disrupt motor control and activation timing of muscles. Additionally, shortened muscles will increase afferent information input via stretch receptors. This in turn contributes to alter motor control through altering muscles primary sensory mechanism – proprioception10. The motor control deficits experienced by the shortened muscles eventually leads to the breakdown of muscle protein via catabolic enzymes and atrophy of the muscle11.
The anatomical, biochemical, and physiological alterations contribute to abnormal segmental control. Having the range of peak force distributed unevenly across a joint alters the load displacement curve. The altered force distribution will put the joint out of a neutral zone creating instability1 (See Figure 2). It should be apparent how the function of muscle changes creating dysfunctional movement through altered synergistic and antagonistic muscle structures. Furthermore, the importance in optimizing proper length tension relationships should be highlighted through the degradation of function in length changes. The process is a cascade of events leading to faulty movement patterns and ultimately structural pathology. Also, it should be noted that the muscular imbalances force the body to compensate and invoke further imbalances within the kinetic chain (ie. Muscular imbalance in shoulder leads to imbalance lumbo-pelvic hip complex). Thus, development of imbalances is a dynamic process that progressively worsens if not corrected.
|
Lengthened Muscle |
Shortened Muscle |
Anatomical Changes |
- Increase Sarcomeres Number Per Fiber
- Decrease in Sarcomere Length
|
- Decrease Sarcomere Number Per fiber
- Increase in Sarcomere Length
|
Biochemical Changes |
|
- Decreased Muscle Weight
- Breakdown of Proteins
|
Physiological Changes |
- Increased Peak Tension
- Altered Peak Tension Range
|
- Decreased Peak Tension
- Altered Peak Tension Range
|
TABLE 2: Summary of Length Associated Changes in Muscle
In conclusion, muscle balance is essential for normal movement. Optimizing functional capacity requires ridding the body of length-associated changes of muscle. Preventative action can be achieved through adopting a mindset of the body is constantly being training by the postures you maintain. Also, existing imbalances can be ridden through establish proper length tension relationships.
REFERNCES
- Comerford MJ, Mottram SL. Movement and stability dysfunction–contemporary developments. Manual therapy. 2001;6(1):15-26.
- Kendall FP, McCreary EK, Kendall HO. Muscles: testing and function. Williams & Wilkins Baltimore, MD; 1983.
-
Janda V, Frank C, Liebenson C. Evaluation of muscular imbalance. Rehabilitation of the Spine: A Practitioner’s Manual. 1996.
- Sahrmann S. Diagnosis and treatment of movement impairment syndromes. Mosby; 2005.
- Page P, Frank C, Lardner R. Assessment and treatment of muscle imbalance: The Janda Approach 2010. Champaign, IL: Human Kinetics.
- Kibler WB. The role of the scapula in athletic shoulder function. The American Journal of Sports Medicine. 1998;26(2):325.
- Gossman MR, Sahrmann SA, Rose SJ. Review of length-associated changes in muscle. Physical Therapy. 1982;62(12):1799-1808.
- Williams P, Goldspink G. Changes in sarcomere length and physiological properties in immobilized muscle. Journal of Anatomy. 1978;127(Pt 3):459.
- McArdle WD, Katch FI, Katch VL. Exercise physiology: nutrition, energy, and human performance. Lippincott Williams & Wilkins; 2009.
- Norris CM. Spinal Stabilisation:: 4. Muscle Imbalance and the Low Back. Physiotherapy. 1995;81(3):127-138.
- Sohar I, Takacs O, Guba F. The influence of immobilization on soluble proteins of muscle. Acta biologica et medica Germanica. 1977;36(11-12):1621-1624.
About the Author
Jason Martuscello, NPI-Certified
Posture Specialist™, is finishing up his M.S. in Exercise Science at
the University of South Florida in Tampa, Florida. He has received his
B.A. from the State University of New York at Plattsburgh. His graduate
research interests include kinesiology, with a specialization in
posture and body alignment. Jason is the Assistant Director of Academic
Relations for the National Posture Institute, in committing to
providing an educational and research based standard in the health and
fitness field. At the University of South Florida, he is a Teaching
Assistant for PET3312 Biomechanics and a Research Assistant. His extra
time is spent volunteering for the federally granted research study in
targeting exercises for preventing back injuries in firefighters. He is
also member of American College of Sports Medicine (ACSM).
|