The Upper Core Part I: Anatomical Considerations
Brushing your teeth, combing your hair and
changing a light bulb may seem like relatively simple common household
tasks. However, simplicity can largely be contributed to the intricate
relationship of the scapula and the shoulder complex. Although large
attention is placed on the trunk (core stability) in training,
rehabilitation and performance in other regions, especially the shoulder
complex, often get overlooked. The shoulder complex plays an integral
role in upper quarter function and deserves more attention. A healthy
shoulder complex will allow ease in functional tasks, better performance
in sporting events, and prevention of injuries. In this Part I series
on the Upper Core, essential anatomical features will be explained.
Also, muscles actively contributing to the mechanics of the upper
quarter region will be considered. The importance will be reinforced
through the pathomechanics of the upper core. The Part II series to the
Upper Core will look at activation and maintenance, through
strengthening to provide stability for upper quarter function.
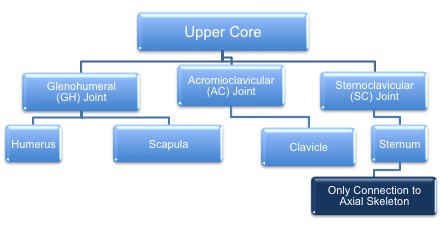
What is the Shoulder Complex?
The
shoulder complex includes the clavicle, scapula, and humerus. The
bones are united through the glenohumeral (GH) and acromioclavicular
(AC), and the sternoclavicular (SC) joints. The scapulothroacic joint
is also included within anatomical descriptions of the upper quarter(1).
Movement
stemming from the upper extremities involves a coordinated interaction
from all the joints. The upper core has unique mechanics that allow
tremendous mobility requiring coordinated and synchronous motion of all
the joints. However, the range of motion is compromised by its lack of
bony or ligamentous attachments from the scapula to the axial
skeleton(2). Due to anatomical architecture, scapulothoracic motion
requires a combination of clavicle motion on the thorax (SC Joint),
and/or further scapula motion relative to the clavicle at the AC
joint(3).
Scapula
The
scapula, often discounted in training programs, bears significant
responsibility in upper quarter function. With numerous muscular
attachments, the scapula work synchronously with the humerus to allow
full range of motion known as scapulohumeral rhythm(4). Through precise
coordination with arm movement, stability is provided for distal
mobility. Another important function is its ability to regulate force
transmission. Through the large range of motion, the scapula prevents
impingement and still allows high force transmission.
Scapula at Rest
The
triangular scapula is a flat bone that lies over the posterior thorax
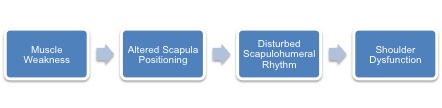
from ribs two to seven. At rest, scapular positioning is important in a
normal functioning upper core. Altered cervical and thoracic spinal
alignment has been postulated in disrupting the resting position
resulting in muscular weakness, dysfunction, and decreased range of
motion(3). One study demonstrated these changes through measuring
spinal posture and its relationship to angulation of the scapula.
Results showed increased forward angulation of the scapula with the
increased curvature of the thoracic spine (kyphotic curve)(3).
Consequently, it is important to assess scapular position during rest.
| The
illustration of father and son raising a heavy ladder can be similar to
the relationship of the muscles of the shoulder. The stronger father
will lift and move the heavy ladder while the weaker son will guide it
as it is raised and prevent it from lifting off the ground (stabilize).
The father represents the static stabilizing muscles (serratus anterior,
trapezius, rhomboids) acting as primary movers and the son acts as the
dynamic stabilizing rotator cuff muscles through stabilization. At any
point the father can generate too much power that will overcome the
resistance of the son resulting in instability(1). |
 |
Summary
The
four joints including the glenohumeral (GH), acromioclavicular (AC),
sternoclavicular (SC), and scapulothoracic make up the upper core.
Normal upper core function requires coordination between joints.
Muscular attachments including the static stabilizers (rhomboids,
trapezius, and serratus anterior) that provide the movement while the
opposing rotator cuff muscles (dynamic stabilizers) maintain stability.
The force couple relationships properly align the bony architecture
through maintaining posture. Any weakness in the kinetic chain will
create a faulty alignment and predispose injury. Therefore, a static
scapular analysis is vital prior to assessing any dynamic movements.
REFERENCES
- Terry GC, Chopp TM. Functional anatomy of the shoulder. Journal of athletic training. 2000;35(3):248.
- Paine R, Voight M. The role of the scapula. The Journal of orthopaedic and sports physical therapy. 1993;18(1):386.
- Culham E, Peat M. Functional anatomy of the shoulder complex. Journal
of Orthopaedic and Sports Physical Therapy. 1993;18:342-342.
- Voight ML, Thomson BC. The role of the scapula in the rehabilitation of
shoulder injuries. Journal of athletic training. 2000;35(3):364.
- Kibler WB. Role of the scapula in the overhead throwing motion. Contemp Orthop. 1991;22(5):525-532.
|